What is lentigo maligna?
Lentigo maligna is an early stage of melanoma skin cancer. They develop when the skin pigment cells (melanocytes) become cancerous and multiply in an uncontrolled way.
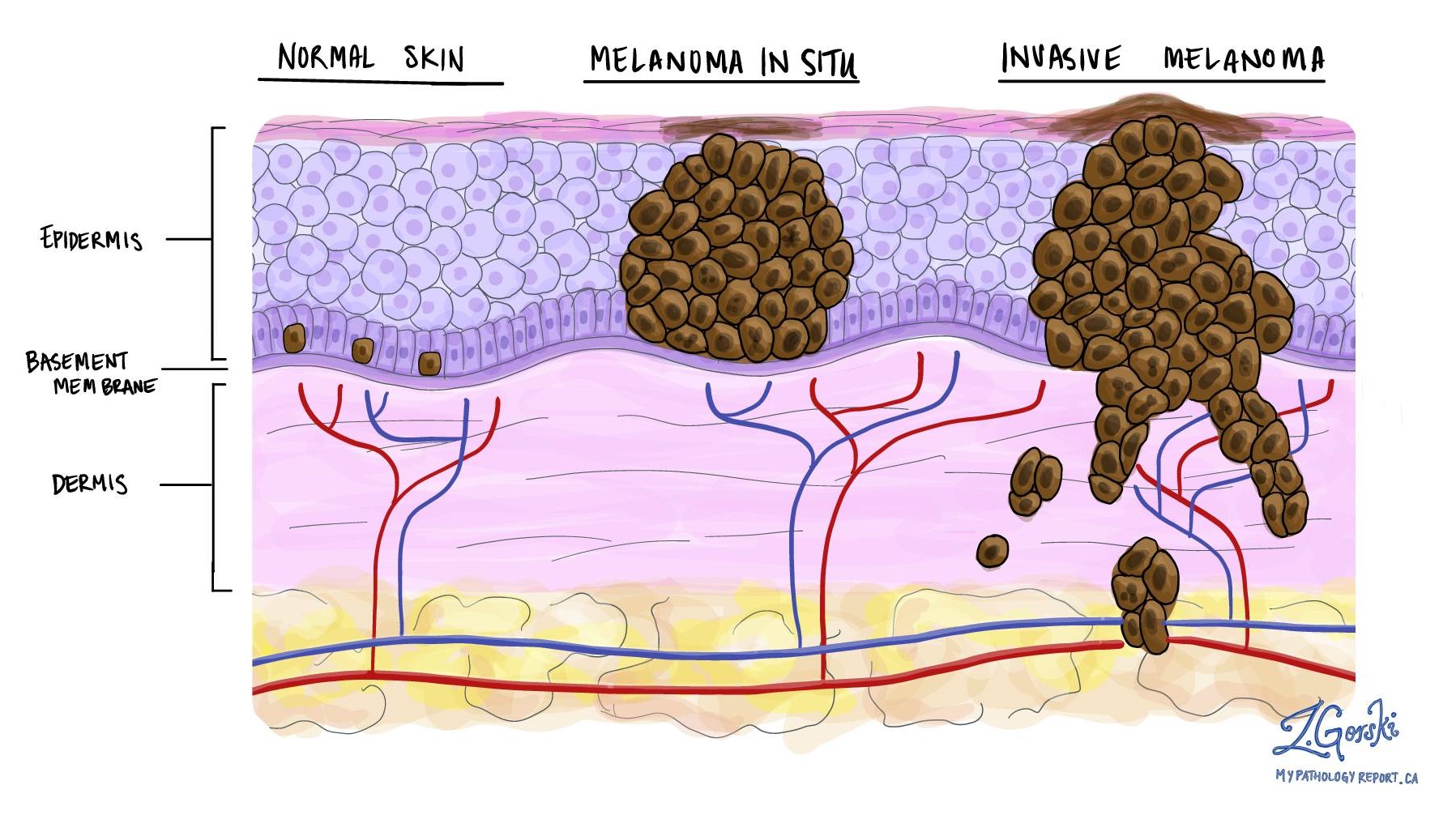
Lentigo maligna is a type of melanoma called ‘in situ’ melanoma. ‘In situ’means that the cancer cells have not had the opportunity to spread anywhere else in the body. There are cancer cells in the top layer of the skin (the epidermis) but they are all contained in the area in which they began to develop. They have not started to spread or grow (‘invade’) into deeper layers of the skin.
Lentigo maligna is a slow growing condition which can take years to develop. It appears in skin that has had a lot of sun exposure, usually the face, neck or upper arms.
Lentigo maligna can be cured with surgery. However, if the whole area is not removed completely with the appropriate surgery, some may develop into an invasive melanoma (Lentigo Maligna Melanoma). They can then invade the skin around them and may also spread to other areas such as the lymph nodes, liver and lungs.
What causes lentigo maligna?
The most important cause is exposure to excessive ultraviolet light in sunlight. It is especially common in fair-skinned people who live in or frequently visit sunny countries. The use of artificial sources of ultraviolet light, such as sunbeds, also raise the risks of melanoma. The risk is increased if another family member has had a melanoma. People who have already had one melanoma have an increased risk of getting another one. Read more about the dangers of tanning beds.
What are the symptoms of lentigo maligna?
Lentigo maligna appears as a long-standing brown patch, most commonly on the face, which slowly enlarges and develops darker areas. Most in situ (very early) melanomas do not cause any symptoms.
How is the diagnosis of lentigo maligna made?
A dermatologist will examine the area carefully, usually with a magnifying device called a dermatoscope, which is placed on the skin. This will help the dermatologist decide whether the area needs to be looked at more closely under the microscope. This may involve removing the whole area under local anaesthetic (a procedure known as an excision) and sending the tissue to the laboratory to be examined. If the area is too large to remove easily, a sample of it (an incisional biopsy) may be taken. If a lentigo maligna is found, the pathology report will provide information that will help to plan the next step in treatment.
Can lentigo maligna be cured?
Yes, the outlook for lentigo maligna is excellent if completely excised with complete assessment of the excised margin.
How should lentigo maligna be treated?
The main treatment for lentigo maligna is surgical. There is no other treatment of proven benefit and usually no other tests are needed. The American Academy of Dermatology (AAD) and National Comprehensive Cancer Network (NCCN) recommend that Staged Micrographic Excision be considered for Lentigo Maligna (melanoma in situ) and early invasive melanomas on chronically sun exposed areas. This technique provides both complete horizontal histological margin assessment and tissue sparing in cosmetically and functionally sensitive areas and improved cure rates.
Staged Micrographic Excision for Lentigo Maligna / Melanoma in situ / Malignant Melanoma
Staged Micrographic Excision (SME) is a surgical procedure where the melanoma is excised with complete assessment of the margin. It provides higher cure rates than traditional surgery and is therefore recommended as the treatment of choice for melanoma in situ (Lentigo Maligna) and early invasive melanoma of cosmetically and functionally important areas. The procedure also offers a tissue sparing effect and therefore better cosmetic and functional outcomes.
With traditional surgery tumour can be left behind, as the whole cut surface is not evaluated but random areas only (about 1% of the margin). The SME method of processing allows tissue slides to be produced that shows the whole, 100% complete cut surface around the tumour. These slides are then examined by a pathologist and will show very accurately any remaining tumour.
SME is not a one-day procedure as the tissue that is excised needs special overnight staining done to identify any remaining cancer cells
What to expect on the day of surgery:
- With your initial consultation the procedure will be discussed in detail.
- SME is a staged procedure and not completed in one day.
- The excision will be done under local anaesthetic.
- Following the excision of the melanoma the defect will either be closed temporarily with stitches or only covered with a dressing depending on the size and location of the defect.
- You will be discharged home with a dressing that will cover the wound until you return to the day hospital for your reconstruction.
- You will be contacted the next day and informed whether any remaining cancer needs to be excised or if you can proceed with the reconstruction.
- The reconstruction of the defect will only take place once it has been confirmed that the melanoma is completely removed.
- The reconstruction is typically performed under conscious sedation.
- Instruction will be given to you by the reconstructive team regarding wound care and follow-up.